According to the urban dictionary, “Mood Typing” refers to how someone types messages that give a clear message to their current mood or feeling.
For many of us, our fingers seem to be constantly attached to a keyboard. Whether it is wading through the endless supply of email, working on academic writing, or engaging with social media.
I am typing thousands of words every week across multiple contexts. To improve my writing ( and catch myself on those annoying little mistakes!) I have been using a couple of tools to monitor my output.
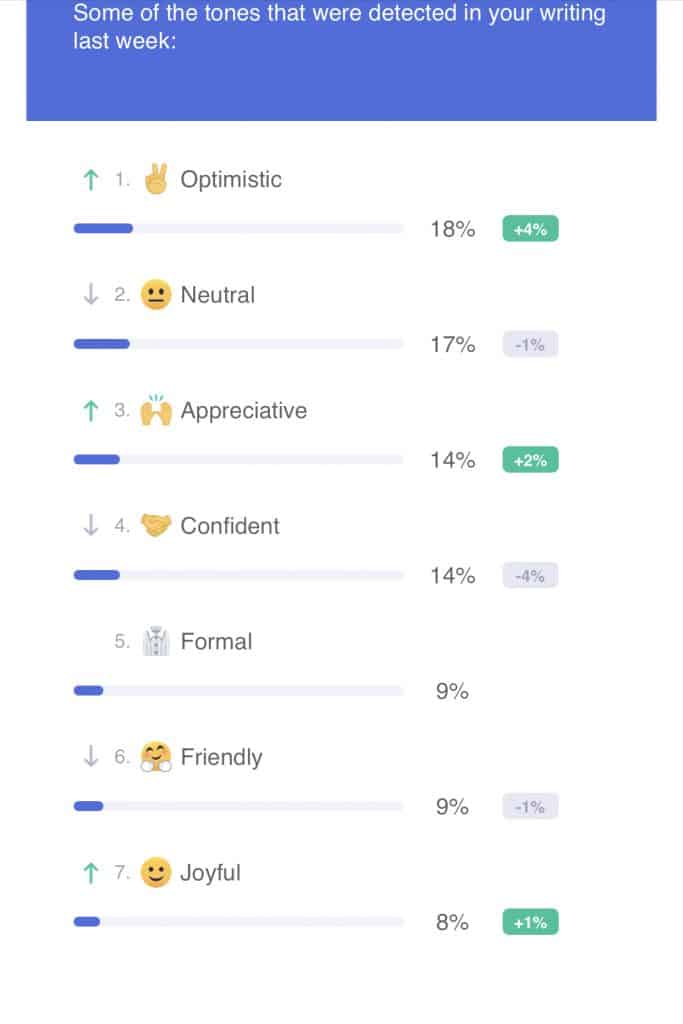
One of the interesting reports that one of these tools emails me each week is a report on the “tones” detected in my writing and the change from week to week.
This weeks report looks like this;
The urban dictionary entry includes this example about mood typing;
“Oh shit, Catleen is angry-typing again. You can tell if she’s pissed at you since she’s always mood-typing.”
It is an interesting exercise each week when this report hits my email to reflect on the week of writing. To consider what has been happening in my various contexts and what might be contributing to the ratio of various tones in my writing.
What tone is happening in your writing? Are you typing up a mood, and what is the reaction of those receiving your writing?
If you want some help, I can recommend using Grammarly (not a sales pitch, no affiliated commissions etc.) It might be interesting to learn about your own writing.
As the program constantly reminds me; To err is human, to edit, divine.
